Article Type: Case Report, Volume 2 Issue 1
*Corresponding author: Mostafa A Mostafa
Neurosurgery Resident, Faculty of Medicine, Al-Azhar University, Cairo, Egypt.
Email: mostafaa02@icloud.com
Received: Mar 25, 2025 Accepted: Apr 14, 2025 Published: Apr 21, 2025
Citation: Mostafa MA, Elsayed MA, Seif B, Mansour LS, Selim H, et al. Repeated hemichorea-hemiballismus as the initial presentation of ketotic hyperglycemia in a 79-year-old female: A case report and literature review. Ann Case Rep Med Images. 2025; 2(1): 1019.
Copyright: Mostafa MA © All rights are reserved
Background: Hemichorea-Hemiballismus (HCHB) is a rare neurological movement disorder characterized by involuntary, violent, jerky movements typically affecting one side of the body, often due to lesions in the basal ganglia from various etiologies.
Case presentation: We report the case of a 79-year-old female with recurrent episodes of involuntary movements on her right side, primarily involving the arm more than the leg, over a three-day period. She had a similar episode one month prior. Initial investigation revealed a Random Blood Sugar (RBS) level of 445 mg/dL and positive urine acetone (+2). Brain Magnetic Resonance Imaging (MRI) shows hyperintensities in the left basal ganglia, consistent with a metabolic insult. The patient had a history of hypertension, for which she was noncompliant with treatment, and hyperlipidemia. She had no prior diagnosis of diabetes mellitus, which was incidentally discovered during this admission, with hemiballismus being her first manifestation of the disease. Neurological examination showed right-sided weakness (grade 4), hypesthesia, upper motor neuron signs, and mild dysarthria. She was fully conscious, with a Glasgow Coma Scale (GCS) score of 15/15 and intact baseline mental status. Management involves achieving optimal glycemic control, along with the use of risperidone, an anti-dopaminergic agent, and clonazepam, a benzodiazepine, to manage symptoms for six weeks. On follow-up in the outpatient clinic, her symptoms were well-controlled, allowing her to transition to monotherapy with risperidone, on which she remained symptomfree in subsequent visits.
Conclusion: HCHB is a rare neurological complication that can arise from uncontrolled diabetes mellitus. While nonketotic hyperglycemia is a more common cause, physicians should consider hemiballismus in the differential diagnosis of patients with hyperglycemia, regardless of ketosis. Prompt diagnosis, exclusion of other common causes, and effective diabetes management can lead to favorable outcomes and help prevent more serious neurological complications.
Keywords: Ketotic hyperglycemia; Uncontrolled diabetes mellitus; Chorea hyperglycemia basal ganglia syndrome; Hemichorea-hemiballismus; Hyperglycemic hemichorea.
Abbreviations: HCHB: Hemichorea-Hemiballismus; RBS: Random Blood Sugar; MRI: Magnetic Resonance Imaging; GCS: Glasgow Coma Scale; CT: Computed Tomography; STN: Contralateral Subthalamic Nucleus; HIV: Human Immunodeficiency Virus; GABA: Gamma-Aminobutyric Acid; SSRIs: Selective Serotonin Reuptake Inhibitors.
Hemichorea-Hemiballismus (HCHB) is a rare, hyperkinetic neurological movement disorder presenting with continuous, irregular, and involuntary movements that affecting one side of the body. Hemiballismus usually arises from a lesion in or near the contralateral Subthalamic Nucleus (STN) [1], with stroke being the most common cause. However, the recent literature has broadened this list of etiologies to include non-ketotic hyperglycemia and complications linked to Human Immunodeficiency Virus (HIV) infection [2].
Diabetes has an age-standardized prevalence of 6.1% worldwide, with the greatest rates (9.3%) occurring in the Middle East and North Africa. In 2021, type 2 diabetes accounted for 95.4% of Diabetes-Related Disability-Adjusted Life Years (DALYs) and 96.0% of cases globally [3]. Considered the most severe type of chorea, hemiballismus is a very rare hyperkinetic movement disorder. It is more commonly linked to non-ketotic hyperglycemia, old age, and female gender, with an estimated global incidence ranging from 1 to 2 per 1,000,000 [4].
Building on this link between diabetes and HCHB, the most frequent cause of the disorder remains stroke in the contralateral striatum or STN. Other causes include encephalitis, neurodegenerative diseases, tumors, medications, ipsilateral chronic subdural hemorrhage, and metabolic disorders like non-ketotic/ketotic hyperglycemia, which is seen in type 2 diabetic patients. In type 2 diabetes, it may be the initial presentation of hyperglycemia [4].
Although HCHB can be severely debilitating, the prognosis is generally favorable, as symptoms often resolve after normalization of blood glucose levels [1]. Here, we report the case of a 79-year-old female who presented with right-sided involuntary movements, which improved with insulin therapy. This case would give insight into the understanding of hemiballismus associated with hyperglycemia, especially in the scenario of ketotic hyperglycemia.
Non-ketotic hyperglycemic chorea-ballismus is a rare but important cause in patients with poorly controlled diabetes mellitus. This case illustrates an unusual cause of movement disorder associated with ketotic hyperglycemia. The prognosis is good, as adequate glycemic control can reverse chorea-ballismus and prevent further neurological complications. Whereas most of the previous cases have been related to long-standing poorly controlled diabetes, our case is notable for presenting hemiballismus as the initial manifestation of diabetes mellitus.
Patient demographics
A 79-year-old female presented to the emergency department complaining of involuntary right-sided movements, predominantly affecting the arm more than the leg, lasting for three days. She had experienced a similar, shorter episode one month prior that resolved within a day.
Medical history
The patient’s medical history included long-standing hypertension, for which she was non-compliant with treatment, and hyperlipidemia. She had no previous diagnosis of diabetes mellitus; however, diabetes was incidentally identified during this admission, with hemiballismus as her initial manifestation.
Presenting symptoms and signs
The patient reported involuntary, non-rhythmic movements of right arm and leg, with the arm being more affected. The movements were of moderate to large amplitude, occurring during rest, postural maintenance, and voluntary actions. She also experienced mild dysarthria and right-sided weakness graded at 4/5, with associated hypesthesia, which had persisted for three days.
Diagnostic workup
Blood tests: Random Blood Sugar (RBS) was 445 mg/dL, and
urine ketones were +2.
Neurological examination: The patient was wide awake, GCS 15/15 with no obvious baseline cognitive impairment. Grading of motor weakness on right side was 4/5 and hypesthesia on the same side consistent with upper motor neuron dysfunction. Mild dysarthria but not significantly impeding her communication.
Her speech was stumbling, non-fluent, and labored without demonstrating paraphrastic errors. With all these difficulties, she succeeded in identifying the most common objects and reading short phrases. Following commands could also be well-performed after some delays, but in recalling the events, at least one out of three showed her minimal disturbances to memory impairment.
Examination of the cranial nerves II through XII showed no deficits. Basic sensory modalities as well as motor strength were relatively preserved. The difficulty letting her extremities relax on examination; however, deep tendon reflexes always 2/4. Without evidence of clonus and with a negative Babinski reflex consistent with no acute upper motor neuron pathology.
Imaging: Initial CT shows a hyperdense lesion strip form in the basal ganglia, which extends the striatopathy in the basal ganglia (Figure 1). Flair-weighted MRI brain shows hypointensity of the left corpus striatum due to basal ganglia affection from diabetes mellitus; T1-weighted MRI of the brain shows hyperintensity of the left basal ganglia, indicating striatopathy of the left basal ganglia due to diabetes mellitus (Figure 2).
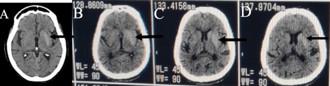
Figure 1: Initial brain Computed Tomography (CT). (A) Hyperdense lesion strip form in basal ganglia; (B-D) Extent of striatopathy in basal ganglia.

Figure 2: (A-B) Flair-weighted MRI showing hypointensity of the left corpus striatum due to basal ganglia affection from diabetes mellitus; (C-D) T1-weighted MRI of the brain showing hyperintensity of the left basal ganglia, indicating striatopathy of the left basal ganglia due to diabetes mellitus.
The differential diagnosis
The differential diagnosis for the patient’s condition includes stroke, other movement disorders such as Huntington’s disease, and hyperosmolar hyperglycemic state without ketosis.
Management and outcome
Effective glycemic management successfully reversed the ketotic hyperglycemic (HCHB) during the patient’s hospital stay. The patient was treated with the anti-dopaminergic medication risperidone and the benzodiazepine clonazepam for six weeks. At her follow-up appointment in the outpatient clinic, she reported that her symptoms were well-controlled with this treatment. Consequently, she was transitioned to monotherapy with risperidone. After six weeks of treatment, we stopped giving the patient the medication, and she remained stable during subsequent follow-up visits.
Outcomes and follow-up
During her hospital stay, the hyperglycemic state was reversed, and hemiballismus symptoms improved significantly, at her follow-up appointment, the patient reported well-controlled symptoms. She was transitioned to monotherapy with risperidone.
After six weeks, medication was discontinued, and she remained symptom-free during subsequent follow-ups.
Several reports have documented cases of individuals with diabetes mellitus or non-ketotic hyperglycemia, caused by uncontrolled blood glucose levels, who experienced acute or subacute onset of hemiballism and choreiform movements during hyperglycemic episodes. Evidence from approximately 200 reported cases of non-ketotic hyperglycemia has shown that most patients were elderly women with a mean age of 71 years, predominantly from East Asia [5,6]. These patients typically exhibit blood glucose levels above 400 mg/dL, negative blood ketones, and imaging findings showing a hyperintense signal in the striatum on MRI or a hyperdensity in the contralateral striatum on CT [7,8]. Despite this, our case presented with +2 ketones in urine, highlighting the rarity of hemiballismus associated with ketotic hyperglycemia, though it remains a possible occurrence.
Initial brain CT is essential to exclude other causes, such as stroke [9]. However, the gold standard for diagnosing hemiballismus is T1-weighted MRI, which can show hyperintensities in the contralateral basal ganglia, particularly in the putamen, globus pallidus, and caudate nucleus, without mass effect, edema, or volume loss [10].
Even though neuropathological results differ according to the cause, the aflicted nuclei and pathways within the basal ganglia circuit remain consistent [8]. Stroke is the most common cause of hemiballismus, followed by encephalitis, neurodegenerative disorders, tumors, drug effects, ipsilateral chronic subdural hemorrhage, and metabolic disorders secondary to uncontrolled diabetes, as in our case [4].
In a hyperglycemia state, hemiballismus can be explained by severe hyperglycemia in an uncontrolled patient, which causes hyperviscosity in the blood and may lead to ischemia, as well as decreased basal ganglia production of acetylcholine and Gamma-Aminobutyric Acid (GABA). This disrupts the balance between neurotransmitters and interferes with normal neural impulse transmission [11].
In a hyperglycemic state, metabolic stress and vascular issues disrupt cerebral homeostasis, particularly in the basal ganglia due to its high glucose demand. This disruption leads to excitotoxic metabolite accumulation, such as lactate and glutamate, which cause neuronal dysfunction [4]. When this hyperglycemic state becomes chronic, it also induces microvascular complications, compromising the blood-brain barrier and leading to focal ischemia [12,13]. Additionally, hyperglycemiarelated manganese accumulation in the basal ganglia interferes with dopaminergic neurotransmission, contributing to motor control issues seen in hemiballismus [4,14]. As a result, all these mechanisms contribute to raising thrombotic risks and predispose the basal ganglia to ischemic damage.
There is not definitively a guideline for the treatment of hemiballismus, though the primary approach remains to control hyperglycemia and ensure good hydration. When hyperglycemia is properly managed, symptoms often disappear within two weeks. About 25% of patients respond to glycemic control alone, although some may need additional drugs, including GABA receptor agonists, Selective Serotonin Reuptake Inhibitors (SSRIs), and dopamine-depleting drugs [15].
The most used monotherapy is haloperidol [16]; other options include clonazepam, risperidone, and tetrabenazine. Haloperidol works effectively when used with clonazepam or diazepam [17]. Complete radiological remission can take several months, and neuroleptic medication may not be required, particularly if lentiform lesions are not present [18,19]. Patient age, lentiform involvement, and neuroleptic use are important prognostic factors [18].
HCHB is a rare neurological complication that can arise from uncontrolled diabetes mellitus. While nonketotic hyperglycemia is a more common cause, physicians should consider hemiballismus in the differential diagnosis of patients with hyperglycemia, regardless of ketosis. Prompt diagnosis, exclusion of other common causes, and effective diabetes management can lead to favorable outcomes and help prevent more serious neurological complications.
Ethics approval and consent to participate: This paper is a case study report, so it does not require ethical approval; written informed consent for participation was obtained from the patient.
Consent to publish: Written informed consent for publication of this case report and accompanying images was obtained from the patient.
Availability of data and materials: Authors declare the possibility to provide data if required.
Funding: Authors declare that the paper did not require funding.
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study.
Conflicts of interest: All authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.